[goal: 3] aims to ensure healthy lives and promote well-being for all. COVID-19 took a catastrophic toll on global health. Childhood vaccination rates declined. Tuberculosis deaths rose. Across the world, about 70 percent of the population received at least one dose of the COVID-19 vaccine. Yet in some countries the rate was as low as 0.3 percent.
Millions of people worldwide died due to COVID-19. In addition to the lives lost from the virus, the pandemic made access to healthcare more difficult, especially in the first years and led to additional preventable deaths caused by other illnesses. Essential childhood vaccination rates also decreased, as did diagnosis rates for tuberculosis and access to malaria treatments.
The catastrophic death toll from COVID-19 does not tell the whole story. Studies indicate that, in addition to the fatalities reported by governments and attributed to COVID-19, many more people died in the first two years of the pandemic (2020 and 2021) compared with levels expected based on historical trends.[footnote: WHO, The Economist, IHME] The true number of lives lost from COVID-19 may never be known because of difficulties in determining the cause of many deaths and in collecting accurate data.
The pandemic caused many more deaths than previously expected
Expected deaths from all causes, pre-pandemic (2020-2021)
Source: World Health Organization. [link: https://www.who.int/data/sets/global-excess-deaths-associated-with-covid-19-modelled-estimates Global excess deaths associated with COVID-19 (modeled estimates)].
Models predicted approximately 113 million deaths in 2020 and 2021 in the absence of the pandemic.
The World Health Organization (WHO) has calculated excess mortality during the first two years of the pandemic. Approximately [emphasis: 15 million] more people died in 2020 and 2021 (combined) than had been expected before the pandemic.
The excess mortality represents the difference between the total deaths and the number expected in the absence of the pandemic.[reference: WHO. May 2022. [link: https://www.who.int/data/stories/global-excess-deaths-associated-with-covid-19-january-2020-december-2021 Global excess deaths associated with COVID-19, January 2020 - December 2021].] Excess mortality measures both the direct and indirect impacts of COVID-19.[footnote: The methodology for estimating the excess mortality associated with the COVID-19 pandemic can be found [link: https://www.who.int/publications/m/item/methods-for-estimating-the-excess-mortality-associatedwith-the-covid-19-pandemic here.]]
The excess mortality figures capture: official deaths attributed to COVID-19 and reported to WHO by countries (5.4 million), COVID-19 deaths not reported by countries, and deaths from other diseases/causes, which resulted from the effects of the pandemic on health systems and society (9.4 million).[footnote: The deaths prevented as a result of pandemic measures like mask wearing or reduced travel are subtracted] [reference: WHO. May 2022. [link: https://www.who.int/data/stories/global-excess-deaths-associated-with-covid-19-january-2020-december-2021 Global excess deaths associated with COVID-19, January 2020 - December 2021].]
Six countries (India, Russia, Indonesia, United States, Brazil, and Mexico) accounted for over 60 percent of the [emphasis: total additional deaths] in the first two years of the pandemic.
The [emphasis: excess death rate] (the number of deaths per 100,000 people), a relative measure, as reported by WHO, shows that countries in Latin America and in Eastern Europe, including Peru, Bulgaria, Bolivia, North Macedonia, Russia, and Armenia, had the largest number of deaths relative to their populations.
Peru and Bulgaria had the highest excess death rates, over 400 per 100,000 people. By comparison, India, which had the highest number of total deaths, had an excess death rate of around 170 per 100,000. The Russian Federation, with the second largest total death toll, had the sixth highest excess death rate at 367 per 100,000 people.
Most countries had positive excess mortality (more people died than if the pandemic had not happened).
However, a few places had lower than expected mortality during the same time frame.
Many of the countries with lower than expected (negative) excess mortality rates are small island states, including St. Kitts and Nevis, Grenada, and Palau. Some of these governments imposed strict isolation measures, such as closing borders to prevent the spread of the virus.
New Zealand, Sri Lanka, and Japan, also experienced relative mortality rates that were lower than pre-pandemic estimates. [footnote: Other countries, such as China, experienced the largest health impacts after 2021, and hence will likely have positive excess rates once data for 2022 are available.]
Source: World Health Organization. [link: https://www.who.int/data/sets/global-excess-deaths-associated-with-covid-19-modelled-estimates Global excess deaths associated with COVID-19 (modeled estimates)].
COVID-19 vaccines have saved many lives
Millions of people died from COVID-19. Had it not been for the vaccines developed beginning in 2020, the death toll would have been even higher. The vaccines are effective at reducing serious illness and death [reference: [link: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines/explainers WHO: Vaccines explained]] and are the first line of defense against the virus.
High and upper-middle income countries have much higher rates of vaccination against COVID-19 than lower-income countries
Source: Our World In Data 2022 [link: https://ourworldindata.org/covid-vaccinations (Mathieu, E., Ritchie, H., Ortiz-Ospina, E. et al. 2021. A global database of COVID-19 vaccinations. Nat Hum Behav.)]
Studies have also estimated how many more people would have died had the vaccines not been made available and how many lives were saved by COVID-19 vaccines in the first year they became available.[footnote: The studies took into account transmission models and vaccine administration.] [reference: The Lancet. [link: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(22)00320-6/fulltext Global impact of the first year of COVID-19 vaccination: a mathematical modelling study].] Results from a Lancet study show that during the first year of immunization against COVID-19 (December 2020 to December 2021) vaccinations prevented at least 14.4 million deaths globally. [footnote: This figure is based on officially reported COVID-19 deaths in 185 countries. When using estimates of total excess mortality, the number of lives saved rises to 19.8 million.]
COVID-19 vaccinations averted millions of deaths
Per-country ratio between COVID-19 deaths averted by vaccination and actual deaths
Source: [link: https://ourworldindata.org/covid-vaccinations Our World In Data 2022] and [link: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(22)00320-6/fulltext Watson et al. 2022 ]
Impact of COVID-19 on global health
One of the aims of [goal: 3] is to end the epidemics of infectious diseases including tuberculosis, malaria, and AIDS by 2030 [target: 3.3]. In recent years, incidence levels for many of these diseases were steadily decreasing. COVID-19 has reversed part of the progress by placing a heavy burden on health systems across the world.
Tuberculosis
The COVID-19 pandemic has led to a setback in progress in reducing tuberculosis (TB). TB is caused by the bacterium, M. tuberculosis, which is transmitted between people through the air when coughing or talking. It is estimated that approximately 1.8 billion people worldwide are infected with M. tuberculosis.[reference: American Lung Association. [link: https://www.lung.org/lung-health-diseases/lung-disease-lookup/tuberculosis/learn-about-tuberculosis#:~:text=About%201.8%20billion%20people%2C%20or,TB%20is%20much%20less%20common Learn About Tuberculosis]. ] Of those infected, only a small percentage of people will develop symptoms (active TB). In its active form, TB causes prolonged cough, chest pain, and coughing up of blood. Active TB can be fatal without treatment.[reference: Centers for Disease Control and Prevention. [link: https://www.cdc.gov/tb/default.htm Tuberculosis]. ] People with weakened immune systems, including those living with HIV, are especially vulnerable to developing active tuberculosis.
Source: World Health Organization. [link: https://www.who.int/publications/i/item/9789240061729 Global tuberculosis report 2022]. Retrieved from World Development Indicators ([link: https://data.worldbank.org/indicator/SH.TBS.INCD SH.TBS.INCD]).
The [emphasis: incidence of tuberculosis] (the number of new and relapsed TB cases per 100,000 people) was highest in South Asia (216) and Sub-Saharan Africa (212) in 2021.
Malnutrition, smoking, and air pollution make tuberculosis more likely to progress from infection to an active form of the disease.[reference: Jassal MS, Bishai WR. 2010. [link: https://academic.oup.com/cid/article/50/Supplement_3/S156/317765 Epidemiology and challenges to the elimination of global tuberculosis.] Clin Infect Dis. 2010 May 15;50 Suppl 3(0 3):S156-64.] Sub-Saharan Africa is particularly vulnerable because of the higher incidence of HIV.[reference: WHO Africa. [link: https://www.afro.who.int/health-topics/tuberculosis-tb Tuberculose] .]
Countries with the highest [emphasis: number of tuberculosis cases] (TB burden) include India, China, Indonesia, Philippines, Pakistan, Nigeria, Bangladesh, Democratic Republic of Congo, and South Africa.
The treatment course for TB takes several months. People living in poverty, without access to adequate health care, have a higher risk of dying from the disease.[reference: Centers for Disease Control and Prevention. [link: https://www.cdc.gov/tb/default.htm Tuberculosis]. ]
During the pandemic, the number of estimated TB cases increased in 2021 for the first time in almost two decades.(You can move the cursor along the timeline to see how the number of cases and incidence change through the years)
Source: World Health Organization. [link: https://www.who.int/publications/i/item/9789240061729 Global tuberculosis report 2022]. Retrieved from World Development Indicators ([link: https://data.worldbank.org/indicator/SH.TBS.INCD SH.TBS.INCD]).
In the years before COVID-19, countries had considerably improved their ability to detect and diagnose TB. In 2020, due to factors including the strain on health systems, fear of catching COVID-19 at health facilities, and other challenges raised by the pandemic, the tuberculosis detection rate [footnote: Tuberculosis case detection rate (all forms) is the number of new and relapse tuberculosis cases notified to WHO in a given year, divided by WHO's estimate of the number of incident tuberculosis cases for the same year, expressed as a percentage.] plummeted around the world. Of the estimated 10 million people who developed TB globally, only 5.8 million were diagnosed in 2020 (compared with 7.1 million in 2019). The number of people diagnosed increased to 6.4 million in 2021.[reference: World Health Organization. [link: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022 Global tuberculosis report 2022]. ]
For example, between 2019 and 2020, the TB detection rate dropped in Serbia from 87 percent to 38 percent, in Italy from 87 percent to 54 percent, and in Jordan from 80 percent to 52 percent, based on data published by WHO. The following year, in 2021, detection rates remained lower than before the pandemic in some regions (Europe & Central Asia, Latin America & Caribbean) or declined further (East Asia & Pacific, North America), while in others (South Asia and Sub-Saharan Africa) detection rates improved.
Tuberculosis detection rates plummeted during the pandemic
Source: World Health Organization. Retrieved from World Development Indicators ([link: https://data.worldbank.org/indicator/SH.TBS.DTEC.ZS SH.TBS.DTEC.ZS]).
The number of deaths from TB increased in the first two years of the pandemic due to limited access to prevention, diagnosis, treatment, and care services. After years of decline, approximately 1.3 million people died of TB in 2020 and 1.4 million in 2021, a level not seen since 2012.
Tuberculosis deaths rose during the pandemic worldwide, as the detection rate decreased
Source: World Health Organization. [link: https://www.who.int/publications/i/item/9789240061729 Global tuberculosis report 2022].
Malaria
[goal: 3] also seeks to end the malaria epidemic by 2030. Malaria is caused by parasites transmitted between humans primarily by infected mosquitoes. The disease causes fever, chills, aches, and in some cases can become severe, leading to coma and death. The risks are especially high for young children, pregnant women, and people without prior exposure to malaria.[reference: Centers for Disease Control and Prevention. [link: https://www.cdc.gov/malaria/about/faqs.html#:~:text=Malaria%20is%20a%20serious%20and,humans%3A%20Plasmodium%20falciparum%2C%20P. Malaria]. ]
Source: World Health Organization. [link: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2022 World malaria report 2022]. Retrieved from World Development Indicators ([link: https://data.worldbank.org/indicator/SH.MLR.INCD.P3 SH.MLR.INCD.P3]).
Malaria can be found in tropical and subtropical countries, and almost half of the global population lives in places where they can be at risk of malaria transmission.[reference: Centers for Disease Control and Prevention. [link: https://www.cdc.gov/malaria/malaria_worldwide/impact.html#:~:text=Africa%20is%20the%20most%20affected,cause%20severe%20malaria%20and%20death. Malaria's Impact Worldwide]. ]
The situation is especially challenging in Sub-Saharan Africa, which has the highest malaria incidence and death rate: over 95 percent of malaria cases and deaths occur in this region.[footnote: In Sub-Saharan Africa, the WHO has certified the following countries as malaria-free: Lesotho, Mauritius, and Seychelles.] This is due to multiple causes including the prevalence of a particularly dangerous type of malaria parasite, weather conditions conducive to transmission, and poverty.
The Democratic Republic of Congo and Nigeria have the largest number of malaria cases. Around 76 percent of people in Nigeria are at risk of contracting the disease.[reference: USAID. [link: https://www.usaid.gov/nigeria/news/eliminating-malaria-nigeria-five-ways-usaids-presidents-malaria-initiative-states-making-difference Eliminating Malaria in Nigeria] .]
During the first year of the COVID-19 pandemic, logistical challenges and higher costs reduced the availability of malaria prevention methods (like insecticides and insecticide-treated bed nets) and medications.
While COVID-19 was spreading around the world, the total number of [emphasis: malaria cases] increased from 232 million in 2019 to 245 million in 2020 – the highest number in ten years. In 2021, malaria cases rose slightly to 247 million.[reference: World Health Organization. [link: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2022 World malaria report 2022]. ] (You can move the cursor along the timeline to see how the number of cases and the incidence change through the years.)
Source: World Health Organization. [link: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2022 World malaria report 2022]. Retrieved from World Development Indicators ([link: https://data.worldbank.org/indicator/SH.MLR.INCD.P3 SH.MLR.INCD.P3]).
After steadily declining for two decades, the number of deaths from malaria rose by about 9 percent to 625,000 in 2020. In 2021, the number decreased only slightly to 619,000.
The increase in cases and deaths can be attributed in part to declines in malaria prevention measures and treatments.[reference: World Health Organization. [link: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2022 World malaria report 2022]. ] These shortfalls led to an increase in both incidence and mortality rates, reversing previous progress. In 2020, mortality rose for the first time in 20 years, and declined slightly in 2021 while remaining above pre-pandemic levels.[footnote: The shortfalls were, nonetheless, less than initially anticipated as countries and donors made concerted efforts to maintain malaria services.]
Malaria mortality rate rose in 2020 for the first time in 20 years
Source: World Health Organization. [link: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2022 World malaria report 2022].
About 80 percent of deaths caused by malaria in Sub-Saharan Africa are among children under five years of age. Older children and adults usually develop some immunity if they live in areas where malaria is prevalent.[reference: World Health Organization. [link: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2021 World malaria report 2021] ]
Malaria disproportionally affects children under 5
Source: World Health Organization. [link: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death Global health estimates: Leading causes of death].
Childhood immunizations
An important aim under [goal: 3] is access to affordable essential medicines and vaccines [target: 3.b]. In many countries, routine childhood vaccination rates fell in 2020 and 2021 because of overburdened medical systems, lockdowns, and fear of COVID-19. These obstacles led to disruptions of important childhood immunization programs such as measles, hepatitis B, and DPT (diphtheria, pertussis/whooping cough, and tetanus).
Many countries experienced drops in childhood vaccination rates in 2020 and 2021
Source: World Health Organization. Retrieved from World Development Indicators ([link: https://data.worldbank.org/indicator/SH.IMM.MEAS SH.IMM.MEAS], [link: https://data.worldbank.org/indicator/SH.IMM.HEPB SH.IMM.HEPB], [link: https://data.worldbank.org/indicator/SH.IMM.IDPT SH.IMM.IDPT]).
23 million children missed out on routine childhood vaccinations in 2020.
Globally, 23 million children missed basic vaccines through routine immunization services in 2020, which is 3.7 million more than in 2019. Most who missed their DPT vaccine in 2020 live in India, Pakistan, and Indonesia, often in remote communities with high levels of poverty.[reference: World Health Organization. 2021. [link: https://www.who.int/news/item/15-07-2021-covid-19-pandemic-leads-to-major-backsliding-on-childhood-vaccinations-new-who-unicef-data-shows COVID-19 pandemic leads to major backsliding on childhood vaccinations]. ]
Number of children not receiving a first dose of diphtheria-tetanus-pertussis combined vaccine (DTP-1)
Source: World Health Organization. 2021. [link: https://www.who.int/news/item/15-07-2021-covid-19-pandemic-leads-to-major-backsliding-on-childhood-vaccinations-new-who-unicef-data-shows COVID-19 pandemic leads to major backsliding on childhood vaccinations].
Barriers to healthcare during the COVID-19 pandemic
Millions of people have died of COVID-19. However, as shown in the beginning of this story, deaths from other causes also increased during the pandemic because of barriers to healthcare access [target: 3.8]. Forgone or delayed care due to health system disruptions (facility closure, insufficient staff, cancellation of elective procedures), fear of becoming infected with COVID-19, mobility restrictions, as well as reduced household incomes contributed to this burden of excess deaths.
Access to healthcare has improved from 2020 to 2021
Percentage of care forgone across country income groups
Source: Kakietek, J., J. Dayton, A. Kerr, and N.K. Stacey. Foregone Healthcare During the COVID-19 Pandemic: 2020 and 2021 Survey Estimates from 25 Developing Countries. Health, Nutrition and Population (HNP) Discussion Paper (Forthcoming). World Bank, Washington, DC.
Household survey data gathered from over 63,000 households across 25 countries [footnote: The data comes from high-frequency poverty survey (HFPS) collected by the World Bank during the COVID-19 to monitor the broad socio-economic impact of the pandemic on households.] over two periods (early days of the pandemic in 2020 and the first half of 2021) show that the overall situation improved in this time frame. In 2020, 18 percent of households reported not being able to access healthcare when needed. The proportion declined to 10 percent in early 2021.[reference: Kakietek, J., J. Dayton, A. Kerr, and N.K. Stacey. Foregone Healthcare During the COVID-19 Pandemic: 2020 and 2021 Survey Estimates from 25 Developing Countries. Health, Nutrition and Population (HNP) Discussion Paper (Forthcoming). World Bank, Washington, DC.]
Financial constraints remained the most commonly reported reason for lack of access to health services. Among households forgoing care, the share who did so for financial reasons was almost the same overall (42 percent in 2020 and 45 percent in early 2021).
During both periods financial barriers were more commonly reported in low and lower-middle income countries. This may be due to the overall higher income levels in upper-middle income countries, but also because financial protection mechanisms are better developed in these economies.
Source: Kakietek, J., J. Dayton, A. Kerr, and N.K. Stacey. Foregone Healthcare During the COVID-19 Pandemic: 2020 and 2021 Survey Estimates from 25 Developing Countries. Health, Nutrition and Population (HNP) Discussion Paper (Forthcoming). World Bank, Washington, DC.
[goal: 3] also seeks to achieve universal health coverage, including financial risk protection, and access to quality essential healthcare services for all [target: 3.8]. Theunequal impact of financial barriers on forgone care highlights the challenges in achieving [target: 3.8]. This situation is particularly worrying given the uneven recovery from the pandemic.
Recent data shows that, as the pandemic has subsided, the economies of richer countries have recovered at a much faster pace than poorer ones (see [goal: 8]). Taking into consideration the additional macroeconomic impact of Russia’s invasion of Ukraine at the global level, the recovery in poorer countries will continue to be slow, financial hardships will persist for a large proportion of households, and many people will forgo healthcare. The disparity between richer and poorer countries in terms of financial barriers to accessing care will likely increase. Therefore, policy actions at the national and global level that ensure financial access to essential health services are critical to sustain progress towards universal health coverage in low and middle-income countries.
Learn more about
SDG
3
In the charts below you can find more facts about SDG {activeGoal} targets, which are not covered in this story. The data for these graphics is derived from official UN data sources.
SDG target
3.8
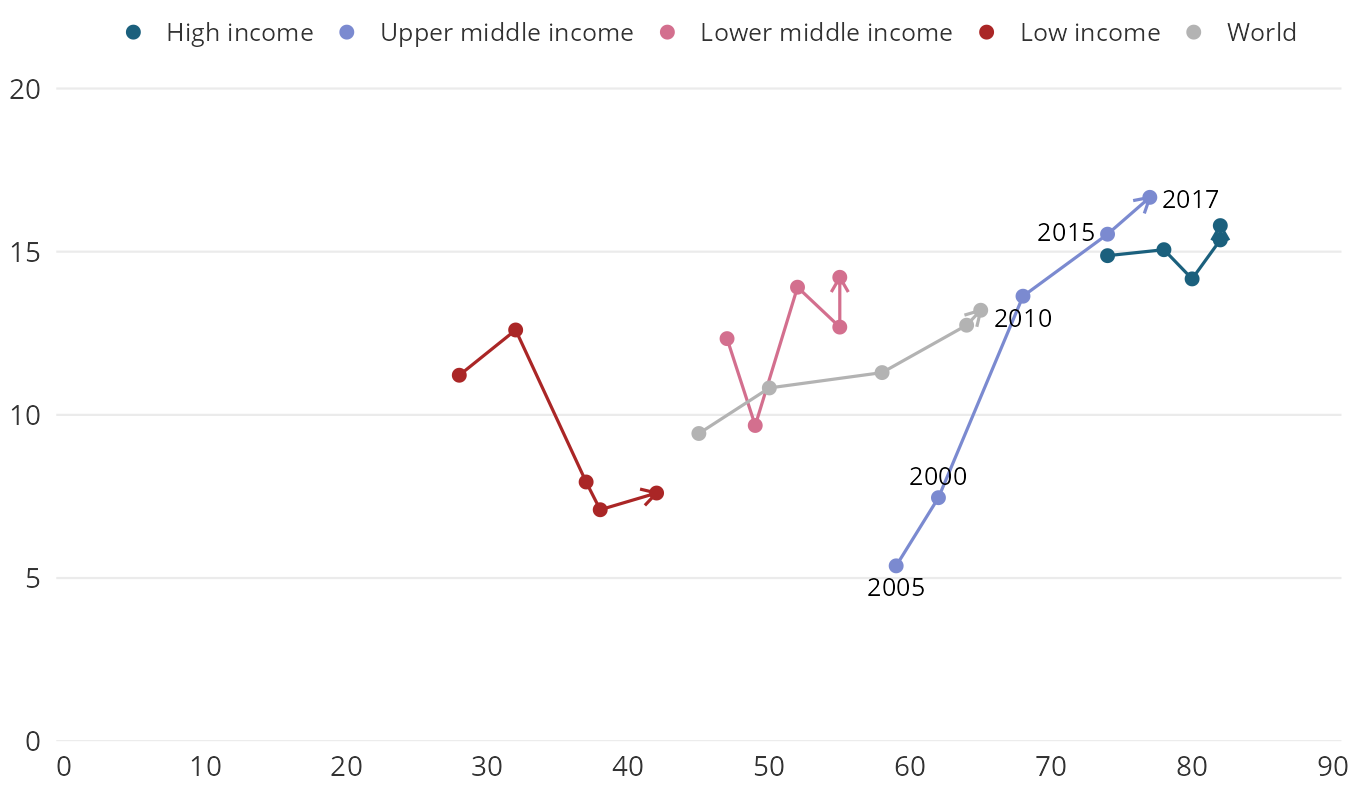
Health service coverage has improved worldwide. However, insufficient social insurance or external support has also increased out-of-pocket healthcare spending.
Trends in UHC (Universal Health Coverage) Service coverage index (x-axis) and proportion of population spending more than 10% of household consumption or income on out-of-pocket healthcare expenditure (y-axis) by income group, 2000-2017
Source: WHO. Retrieved from World Development Indicators ([link: https://data.worldbank.org/indicator/SH.UHC.SRVS.CV.XD SH.UHC.SRVS.CV.XD], [link: https://data.worldbank.org/indicator/SH.UHC.OOPC.10.ZS SH.UHC.OOPC.10.ZS]).DOWNLOAD
SDG target
3.2
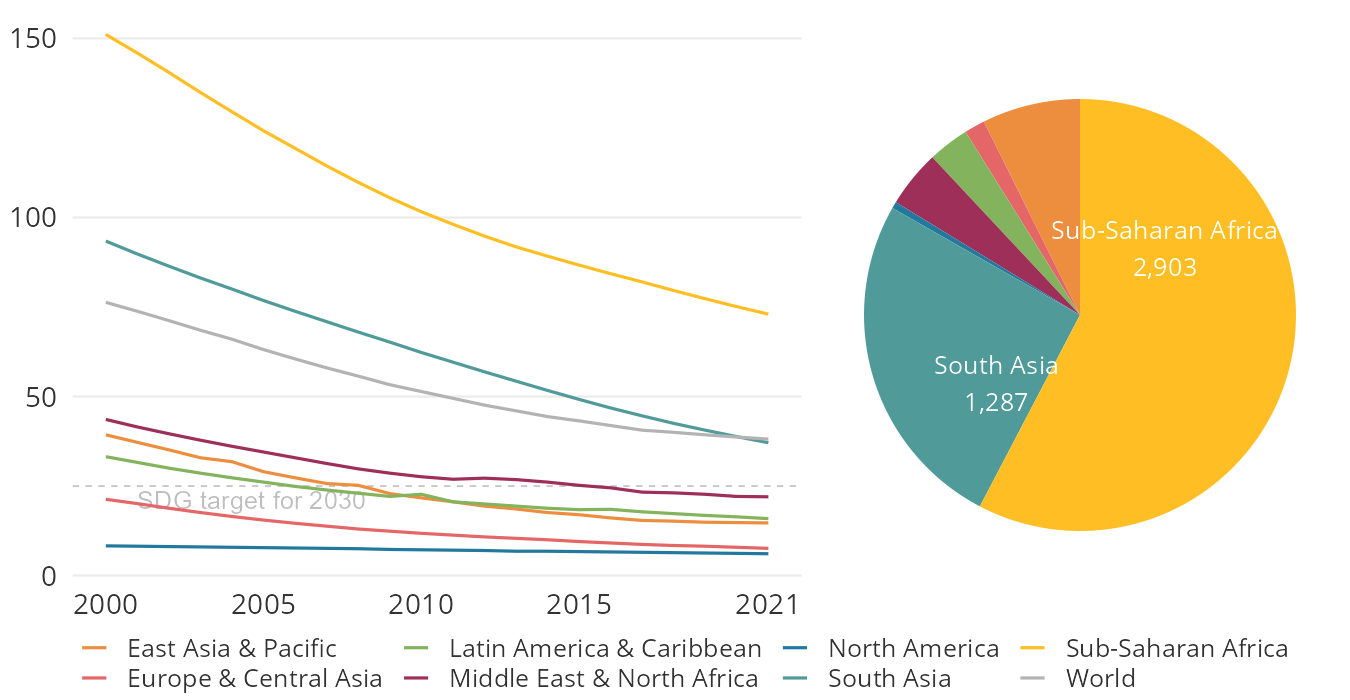
Sub-Saharan Africa and South Asia bear the largest burden of deaths for children under-five.
Under-five mortality rate (deaths per 1,000 live births) by region, 2000-2021 (left) and the number of under-five deaths (in thousands) by region, 2021 (right)
Source: UN Inter-agency Group for Child Mortality Estimation. Retrieved from World Development Indicators ([link: https://data.worldbank.org/indicator/SH.DTH.MORT SH.DTH.MORT], [link: https://data.worldbank.org/indicator/SH.DYN.MORT SH.DYN.MORT]).DOWNLOAD
SDG target
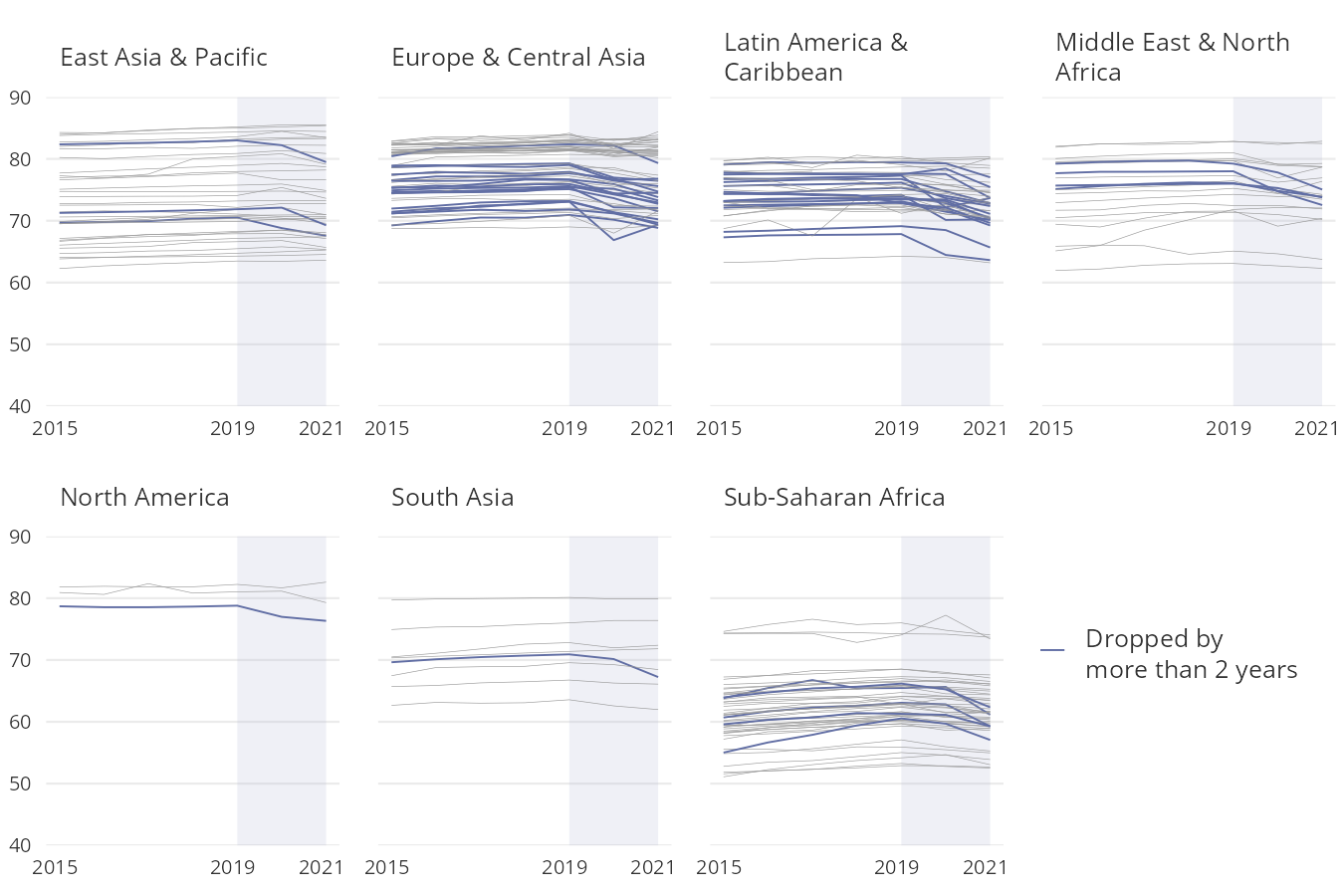
Following the COVID-19 pandemic, life expectancy at birth declined from 2019 to 2021 in more than 70 percent of countries, although the extent varies across regions and countries.
Life expectancy at birth by region (years), 2015-2021
Source: United Nations Population Division. Retrieved from World Development Indicators ([link: https://data.worldbank.org/indicator/SP.DYN.LE00.IN SP.DYN.LE00.IN]).DOWNLOAD
SDG target
3.1
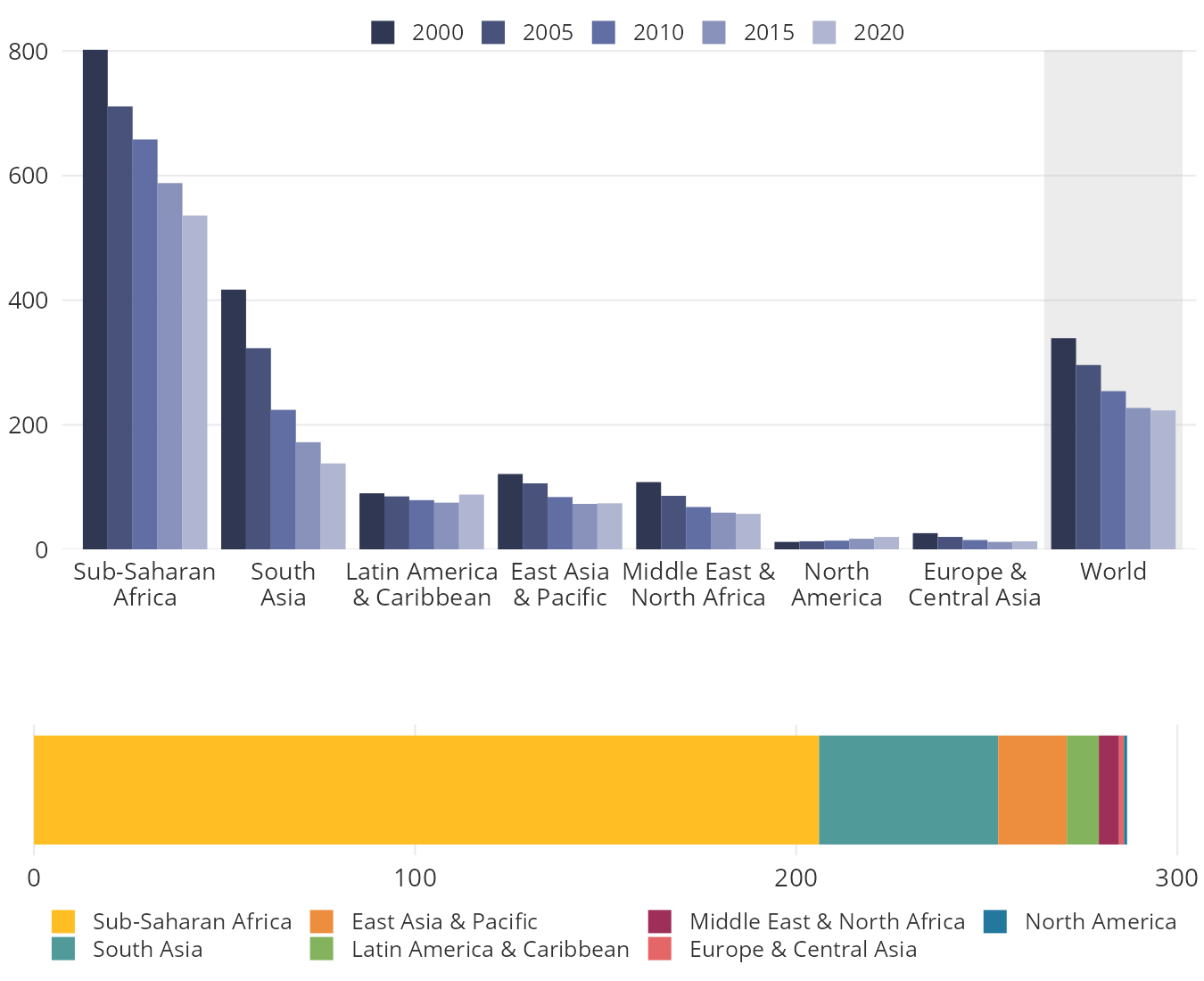
Despite progress, large inequities in maternal survival exist across regions.
Maternal mortality ratio (per 100,000 live births) by region, 2000-2020 (top) and the number of maternal deaths in thousands by region, 2020 (bottom)
Source: United Nations Maternal Mortality Estimation Inter-Agency Group (UN MMEIG). Retrieved from World Development Indicators ([link: https://data.worldbank.org/indicator/SH.STA.MMRT SH.STA.MMRT], [link: https://data.worldbank.org/indicator/SH.MMR.DTHS SP.DYN.LE00.IN]).DOWNLOAD